Request Demo
What is Cangrelor used for?
14 June 2024
Cangrelor is a potent intravenous antiplatelet drug developed to prevent platelet aggregation, thereby reducing the risk of thrombotic cardiovascular events. Known by its trade name Kengreal in the United States and Canada, and Kengrexal in the European market, this drug has been a significant advancement in the field of cardiovascular medicine. Cangrelor targets the P2Y12 receptor on platelets, which plays a crucial role in platelet activation and aggregation. It is primarily indicated for patients undergoing percutaneous coronary intervention (PCI), particularly those at risk of coronary artery thrombosis who have not been pre-treated with an oral P2Y12 inhibitor. The development of Cangrelor involved extensive research and collaboration among several institutions, including The Medicines Company, which spearheaded clinical trials. After years of rigorous testing and validation, Cangrelor received FDA approval in 2015, marking a milestone in the management of acute coronary syndromes.
Cangrelor works by selectively and reversibly binding to the P2Y12 receptor on the surface of platelets. The P2Y12 receptor is essential for the amplification of platelet aggregation in response to adenosine diphosphate (ADP). By inhibiting this receptor, Cangrelor effectively prevents the conformational change and activation of the glycoprotein IIb/IIIa receptor complex, which is necessary for fibrinogen binding and subsequent platelet aggregation. Unlike oral P2Y12 inhibitors such as clopidogrel, prasugrel, and ticagrelor, Cangrelor's intravenous administration allows for a faster onset and offset of action. This rapid pharmacokinetic profile makes it particularly useful in acute settings where immediate platelet inhibition is required, such as during PCI procedures.
Cangrelor is administered intravenously, allowing it to achieve rapid and potent platelet inhibition. The recommended dosing regimen starts with an initial bolus of 30 micrograms per kilogram over one minute, followed by a continuous infusion of 4 micrograms per kilogram per minute. The onset of action is almost immediate, typically within two minutes of administration, providing quick and effective platelet inhibition. The duration of the infusion can be adjusted based on the clinical scenario, but it is generally continued for the duration of the PCI procedure. Due to its short half-life of approximately three to six minutes, the antiplatelet effects of Cangrelor diminish rapidly after the infusion is stopped, with platelet function returning to near baseline levels within an hour. This reversible and controllable pharmacodynamic profile makes Cangrelor a versatile option for managing acute thrombotic risks during and immediately after PCI.
While Cangrelor is generally well-tolerated, it is not without its side effects and contraindications. The most common adverse effect associated with Cangrelor is bleeding, which can range from minor to severe. Major bleeding events, although less common, can include gastrointestinal bleeding, intracranial hemorrhage, and access site bleeding. Other reported side effects include dyspnea, hypotension, and hypersensitivity reactions, although these are relatively rare. Contraindications for Cangrelor use include active pathological bleeding, such as peptic ulcer disease or intracranial hemorrhage, and a history of hypersensitivity to the drug or any of its components. Additionally, Cangrelor should be used with caution in patients with a high risk of bleeding or those with coagulopathies. Monitoring for signs of bleeding during and after treatment is essential to ensure patient safety.
Cangrelor can interact with other medications, potentially altering its effectiveness or increasing the risk of adverse effects. Drugs that affect hemostasis, such as anticoagulants (e.g., warfarin, heparin) and other antiplatelet agents (e.g., aspirin, clopidogrel), can augment the bleeding risk when used concomitantly with Cangrelor. Therefore, careful consideration and close monitoring are required when these drugs are co-administered. Additionally, Cangrelor's antiplatelet effects can interfere with the action of glycoprotein IIb/IIIa inhibitors (e.g., abciximab, eptifibatide), potentially leading to increased bleeding complications. Physicians should be aware of these interactions and adjust treatment protocols accordingly. It is also important to note that transitioning from Cangrelor to oral P2Y12 inhibitors requires careful timing to avoid gaps in platelet inhibition. For instance, clopidogrel and prasugrel should not be administered until Cangrelor infusion is discontinued, while ticagrelor can be given during the Cangrelor infusion or immediately after its cessation to maintain continuous platelet inhibition.
In conclusion, Cangrelor represents a significant advancement in the management of acute thrombotic events in patients undergoing PCI. Its rapid onset and offset of action, coupled with its potent antiplatelet effects, make it an invaluable tool in the cardiovascular arsenal. However, like all medications, it requires careful consideration of its side effects, contraindications, and potential drug interactions to ensure its safe and effective use. As research continues to evolve, Cangrelor's role in cardiovascular medicine will likely expand, offering new therapeutic possibilities for patients at risk of thrombotic events.
Cangrelor works by selectively and reversibly binding to the P2Y12 receptor on the surface of platelets. The P2Y12 receptor is essential for the amplification of platelet aggregation in response to adenosine diphosphate (ADP). By inhibiting this receptor, Cangrelor effectively prevents the conformational change and activation of the glycoprotein IIb/IIIa receptor complex, which is necessary for fibrinogen binding and subsequent platelet aggregation. Unlike oral P2Y12 inhibitors such as clopidogrel, prasugrel, and ticagrelor, Cangrelor's intravenous administration allows for a faster onset and offset of action. This rapid pharmacokinetic profile makes it particularly useful in acute settings where immediate platelet inhibition is required, such as during PCI procedures.
Cangrelor is administered intravenously, allowing it to achieve rapid and potent platelet inhibition. The recommended dosing regimen starts with an initial bolus of 30 micrograms per kilogram over one minute, followed by a continuous infusion of 4 micrograms per kilogram per minute. The onset of action is almost immediate, typically within two minutes of administration, providing quick and effective platelet inhibition. The duration of the infusion can be adjusted based on the clinical scenario, but it is generally continued for the duration of the PCI procedure. Due to its short half-life of approximately three to six minutes, the antiplatelet effects of Cangrelor diminish rapidly after the infusion is stopped, with platelet function returning to near baseline levels within an hour. This reversible and controllable pharmacodynamic profile makes Cangrelor a versatile option for managing acute thrombotic risks during and immediately after PCI.
While Cangrelor is generally well-tolerated, it is not without its side effects and contraindications. The most common adverse effect associated with Cangrelor is bleeding, which can range from minor to severe. Major bleeding events, although less common, can include gastrointestinal bleeding, intracranial hemorrhage, and access site bleeding. Other reported side effects include dyspnea, hypotension, and hypersensitivity reactions, although these are relatively rare. Contraindications for Cangrelor use include active pathological bleeding, such as peptic ulcer disease or intracranial hemorrhage, and a history of hypersensitivity to the drug or any of its components. Additionally, Cangrelor should be used with caution in patients with a high risk of bleeding or those with coagulopathies. Monitoring for signs of bleeding during and after treatment is essential to ensure patient safety.
Cangrelor can interact with other medications, potentially altering its effectiveness or increasing the risk of adverse effects. Drugs that affect hemostasis, such as anticoagulants (e.g., warfarin, heparin) and other antiplatelet agents (e.g., aspirin, clopidogrel), can augment the bleeding risk when used concomitantly with Cangrelor. Therefore, careful consideration and close monitoring are required when these drugs are co-administered. Additionally, Cangrelor's antiplatelet effects can interfere with the action of glycoprotein IIb/IIIa inhibitors (e.g., abciximab, eptifibatide), potentially leading to increased bleeding complications. Physicians should be aware of these interactions and adjust treatment protocols accordingly. It is also important to note that transitioning from Cangrelor to oral P2Y12 inhibitors requires careful timing to avoid gaps in platelet inhibition. For instance, clopidogrel and prasugrel should not be administered until Cangrelor infusion is discontinued, while ticagrelor can be given during the Cangrelor infusion or immediately after its cessation to maintain continuous platelet inhibition.
In conclusion, Cangrelor represents a significant advancement in the management of acute thrombotic events in patients undergoing PCI. Its rapid onset and offset of action, coupled with its potent antiplatelet effects, make it an invaluable tool in the cardiovascular arsenal. However, like all medications, it requires careful consideration of its side effects, contraindications, and potential drug interactions to ensure its safe and effective use. As research continues to evolve, Cangrelor's role in cardiovascular medicine will likely expand, offering new therapeutic possibilities for patients at risk of thrombotic events.
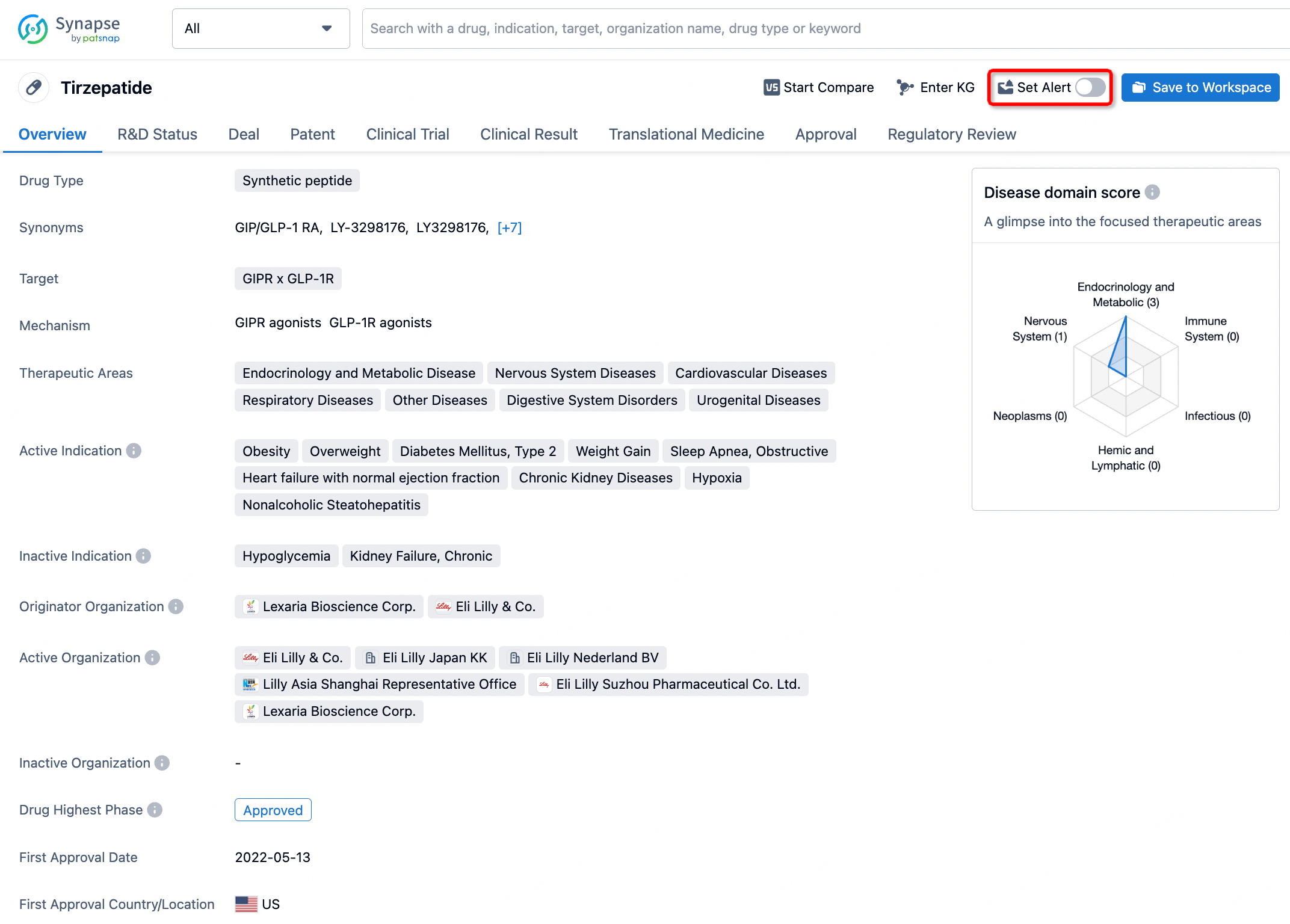
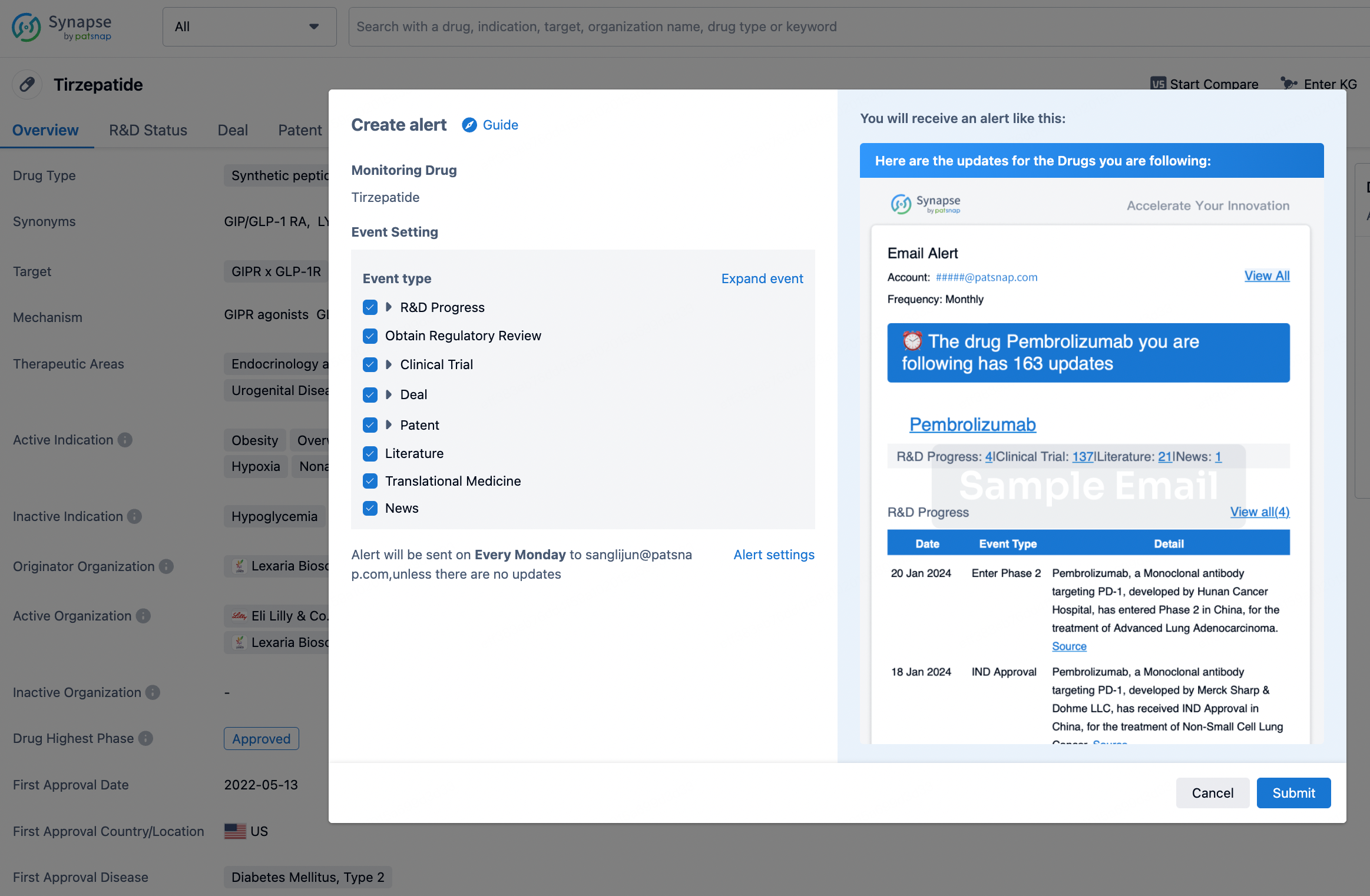
How to obtain the latest development progress of all drugs?
In the Synapse database, you can stay updated on the latest research and development advances of all drugs. This service is accessible anytime and anywhere, with updates available daily or weekly. Use the "Set Alert" function to stay informed. Click on the image below to embark on a brand new journey of drug discovery!
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.