Request Demo
What is Piperacillin Sodium used for?
15 June 2024
Piperacillin Sodium, a vital member of the penicillin family of antibiotics, is known for its broad spectrum of activity against numerous bacterial pathogens. Marketed under various trade names such as Pipracil, it has been a cornerstone in the treatment of severe infections. Its primary targets include a range of Gram-positive and Gram-negative bacteria, including Pseudomonas aeruginosa, which is notoriously difficult to treat. Piperacillin Sodium is often utilized in hospital settings, particularly in intensive care units, to combat severe and life-threatening bacterial infections. Various pharmaceutical research institutions have extensively studied this drug to better understand its efficacy, safety, and the breadth of its antibacterial activity.
This beta-lactam antibiotic is often combined with tazobactam, a beta-lactamase inhibitor, to overcome bacterial resistance mechanisms. The combination, known as Piperacillin/Tazobactam or Tazocin, effectively extends the drug's spectrum of activity. The research progress on Piperacillin Sodium has been significant, with numerous clinical trials demonstrating its efficacy in treating conditions such as intra-abdominal infections, pneumonia, sepsis, and febrile neutropenia. It is recognized as a critical option for patients with severe and complicated infections, often reserved for those who do not respond to other antibiotics.
Piperacillin Sodium exerts its antibacterial effects by inhibiting the synthesis of the bacterial cell wall. The drug binds to penicillin-binding proteins (PBPs) located inside the bacterial cell membrane. PBPs play a crucial role in the final stages of synthesizing and remodeling the bacterial cell wall. By binding to these proteins, Piperacillin Sodium disrupts the cross-linking of peptidoglycan chains, which are essential components of the bacterial cell wall. This inhibition leads to the weakening of the cell wall, causing it to rupture and ultimately resulting in bacterial cell death.
The action of Piperacillin Sodium is bactericidal, meaning it kills bacteria rather than merely inhibiting their growth. This mechanism is particularly effective against rapidly dividing bacteria, which rely heavily on cell wall synthesis. When combined with tazobactam, Piperacillin's efficacy is further enhanced. Tazobactam inhibits beta-lactamase enzymes produced by some bacteria that would otherwise degrade Piperacillin, rendering it ineffective. Thus, the combination therapy provides a robust shield against a broader range of bacterial pathogens, including those that have developed resistance to other antibiotics.
Piperacillin Sodium is typically administered intravenously, ensuring rapid delivery into the bloodstream and quick onset of action. This mode of administration is particularly advantageous in clinical settings where time is of the essence, such as in severe infections. The drug can also be administered intramuscularly, though this route is less common due to the associated pain and variability in absorption.
The dosage and frequency of Piperacillin Sodium administration depend on the severity and type of infection being treated, as well as the patient's renal function. For instance, in adults with normal renal function, typical doses range from 3 to 4 grams every 4 to 6 hours. In cases of severe infections, higher doses may be necessary. Pediatric dosing is usually weight-based, and adjustments are made for patients with renal impairment to prevent drug accumulation and toxicity.
The onset of action for Piperacillin Sodium is relatively swift, with peak plasma concentrations reached within 30 minutes to an hour after intravenous administration. This rapid onset is crucial for treating severe infections, where prompt bacterial eradication can significantly impact patient outcomes. The duration of treatment varies but typically ranges from 7 to 14 days, depending on the clinical response and the pathogen involved.
Like all medications, Piperacillin Sodium can cause side effects, some of which may be severe. Common side effects include gastrointestinal disturbances such as nausea, vomiting, diarrhea, and abdominal pain. These symptoms are generally mild and transient. However, more serious adverse effects can occur, necessitating close monitoring during treatment.
Hypersensitivity reactions, including rash, pruritus, and fever, are relatively common. In rare cases, more severe allergic reactions such as anaphylaxis may occur, necessitating immediate medical intervention. Patients with a history of penicillin allergy should avoid using Piperacillin Sodium unless absolutely necessary and should be closely monitored if no alternatives are available.
Hematologic side effects, including neutropenia, thrombocytopenia, and eosinophilia, have been reported. These conditions warrant regular blood count monitoring to detect any abnormalities early. Hepatotoxicity, manifested as elevated liver enzymes, is another potential side effect, particularly with prolonged use. Renal function should also be monitored, especially in patients with preexisting kidney disease, as Piperacillin can cause interstitial nephritis.
Neurological side effects such as seizures and encephalopathy can occur, particularly in patients with renal impairment receiving high doses. As such, dose adjustments are crucial in these populations. Additionally, electrolyte imbalances, specifically hypokalemia, may occur, requiring regular monitoring of serum potassium levels.
Certain drugs can interact with Piperacillin Sodium, potentially altering its effectiveness or increasing the risk of adverse effects. One significant interaction is with aminoglycoside antibiotics, such as gentamicin. While these drugs are often used together to treat severe infections, they should not be mixed in the same intravenous solution due to chemical incompatibility. Instead, they should be administered separately.
Probenecid, a medication used to treat gout, can affect Piperacillin Sodium by decreasing its renal excretion, leading to higher plasma levels and an increased risk of toxicity. Concomitant use of anticoagulants, such as warfarin, with Piperacillin may increase the risk of bleeding. This interaction necessitates close monitoring of coagulation parameters to adjust the anticoagulant dose if necessary.
Other antibiotics such as tetracyclines and chloramphenicol can antagonize the bactericidal effects of Piperacillin Sodium, potentially reducing its efficacy. Therefore, combining these drugs should be avoided. Additionally, the use of nonsteroidal anti-inflammatory drugs (NSAIDs) may increase the risk of nephrotoxicity when used with Piperacillin, particularly in patients with preexisting renal conditions.
In conclusion, Piperacillin Sodium is a potent and versatile antibiotic essential in treating severe and complicated bacterial infections. Its broad-spectrum activity, particularly when combined with tazobactam, makes it a valuable tool in combating antibiotic-resistant bacteria. Understanding its mechanism of action, appropriate usage, potential side effects, and drug interactions is crucial for healthcare providers to optimize treatment outcomes and ensure patient safety.
This beta-lactam antibiotic is often combined with tazobactam, a beta-lactamase inhibitor, to overcome bacterial resistance mechanisms. The combination, known as Piperacillin/Tazobactam or Tazocin, effectively extends the drug's spectrum of activity. The research progress on Piperacillin Sodium has been significant, with numerous clinical trials demonstrating its efficacy in treating conditions such as intra-abdominal infections, pneumonia, sepsis, and febrile neutropenia. It is recognized as a critical option for patients with severe and complicated infections, often reserved for those who do not respond to other antibiotics.
Piperacillin Sodium exerts its antibacterial effects by inhibiting the synthesis of the bacterial cell wall. The drug binds to penicillin-binding proteins (PBPs) located inside the bacterial cell membrane. PBPs play a crucial role in the final stages of synthesizing and remodeling the bacterial cell wall. By binding to these proteins, Piperacillin Sodium disrupts the cross-linking of peptidoglycan chains, which are essential components of the bacterial cell wall. This inhibition leads to the weakening of the cell wall, causing it to rupture and ultimately resulting in bacterial cell death.
The action of Piperacillin Sodium is bactericidal, meaning it kills bacteria rather than merely inhibiting their growth. This mechanism is particularly effective against rapidly dividing bacteria, which rely heavily on cell wall synthesis. When combined with tazobactam, Piperacillin's efficacy is further enhanced. Tazobactam inhibits beta-lactamase enzymes produced by some bacteria that would otherwise degrade Piperacillin, rendering it ineffective. Thus, the combination therapy provides a robust shield against a broader range of bacterial pathogens, including those that have developed resistance to other antibiotics.
Piperacillin Sodium is typically administered intravenously, ensuring rapid delivery into the bloodstream and quick onset of action. This mode of administration is particularly advantageous in clinical settings where time is of the essence, such as in severe infections. The drug can also be administered intramuscularly, though this route is less common due to the associated pain and variability in absorption.
The dosage and frequency of Piperacillin Sodium administration depend on the severity and type of infection being treated, as well as the patient's renal function. For instance, in adults with normal renal function, typical doses range from 3 to 4 grams every 4 to 6 hours. In cases of severe infections, higher doses may be necessary. Pediatric dosing is usually weight-based, and adjustments are made for patients with renal impairment to prevent drug accumulation and toxicity.
The onset of action for Piperacillin Sodium is relatively swift, with peak plasma concentrations reached within 30 minutes to an hour after intravenous administration. This rapid onset is crucial for treating severe infections, where prompt bacterial eradication can significantly impact patient outcomes. The duration of treatment varies but typically ranges from 7 to 14 days, depending on the clinical response and the pathogen involved.
Like all medications, Piperacillin Sodium can cause side effects, some of which may be severe. Common side effects include gastrointestinal disturbances such as nausea, vomiting, diarrhea, and abdominal pain. These symptoms are generally mild and transient. However, more serious adverse effects can occur, necessitating close monitoring during treatment.
Hypersensitivity reactions, including rash, pruritus, and fever, are relatively common. In rare cases, more severe allergic reactions such as anaphylaxis may occur, necessitating immediate medical intervention. Patients with a history of penicillin allergy should avoid using Piperacillin Sodium unless absolutely necessary and should be closely monitored if no alternatives are available.
Hematologic side effects, including neutropenia, thrombocytopenia, and eosinophilia, have been reported. These conditions warrant regular blood count monitoring to detect any abnormalities early. Hepatotoxicity, manifested as elevated liver enzymes, is another potential side effect, particularly with prolonged use. Renal function should also be monitored, especially in patients with preexisting kidney disease, as Piperacillin can cause interstitial nephritis.
Neurological side effects such as seizures and encephalopathy can occur, particularly in patients with renal impairment receiving high doses. As such, dose adjustments are crucial in these populations. Additionally, electrolyte imbalances, specifically hypokalemia, may occur, requiring regular monitoring of serum potassium levels.
Certain drugs can interact with Piperacillin Sodium, potentially altering its effectiveness or increasing the risk of adverse effects. One significant interaction is with aminoglycoside antibiotics, such as gentamicin. While these drugs are often used together to treat severe infections, they should not be mixed in the same intravenous solution due to chemical incompatibility. Instead, they should be administered separately.
Probenecid, a medication used to treat gout, can affect Piperacillin Sodium by decreasing its renal excretion, leading to higher plasma levels and an increased risk of toxicity. Concomitant use of anticoagulants, such as warfarin, with Piperacillin may increase the risk of bleeding. This interaction necessitates close monitoring of coagulation parameters to adjust the anticoagulant dose if necessary.
Other antibiotics such as tetracyclines and chloramphenicol can antagonize the bactericidal effects of Piperacillin Sodium, potentially reducing its efficacy. Therefore, combining these drugs should be avoided. Additionally, the use of nonsteroidal anti-inflammatory drugs (NSAIDs) may increase the risk of nephrotoxicity when used with Piperacillin, particularly in patients with preexisting renal conditions.
In conclusion, Piperacillin Sodium is a potent and versatile antibiotic essential in treating severe and complicated bacterial infections. Its broad-spectrum activity, particularly when combined with tazobactam, makes it a valuable tool in combating antibiotic-resistant bacteria. Understanding its mechanism of action, appropriate usage, potential side effects, and drug interactions is crucial for healthcare providers to optimize treatment outcomes and ensure patient safety.
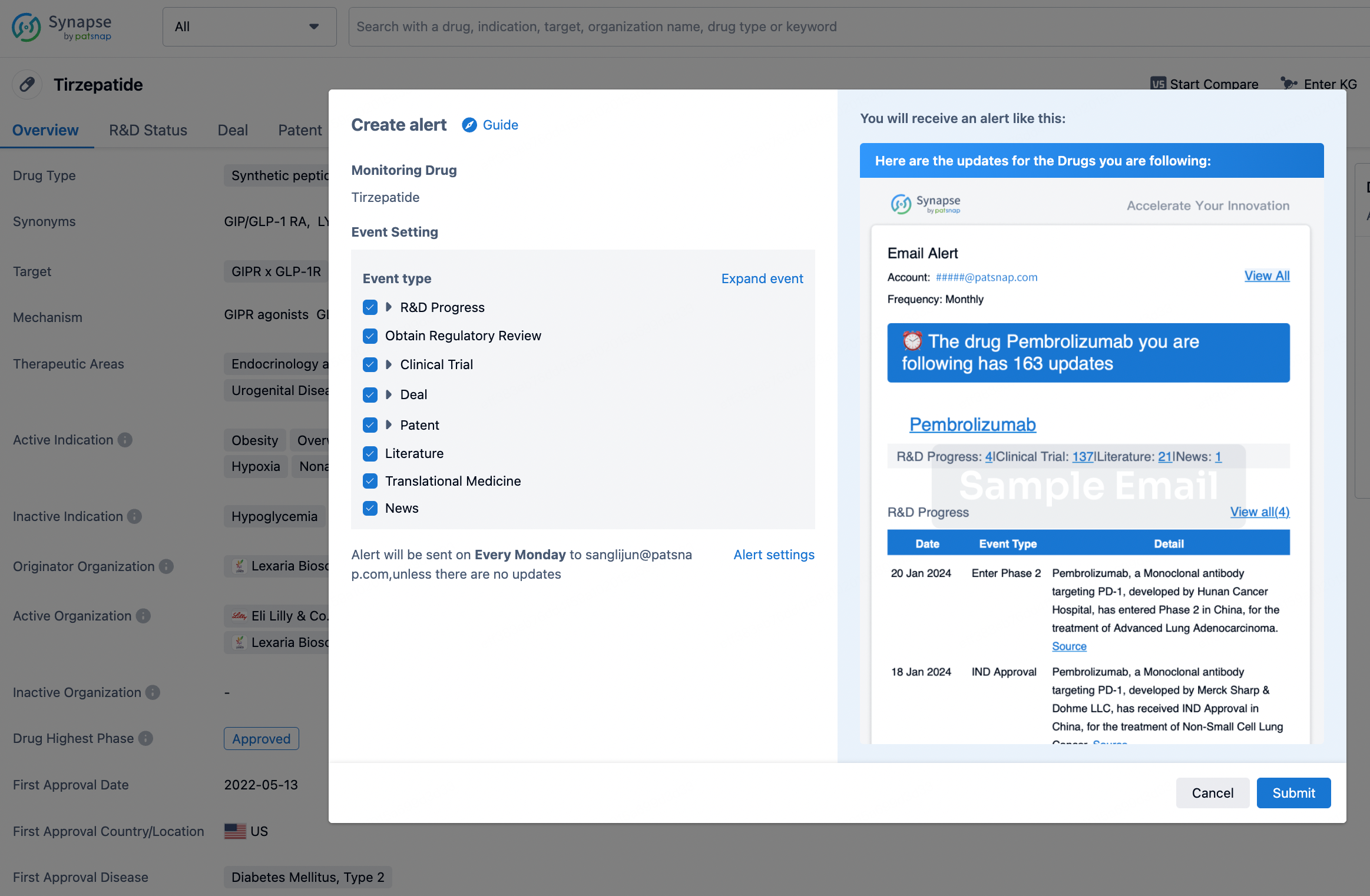
How to obtain the latest development progress of all drugs?
In the Synapse database, you can stay updated on the latest research and development advances of all drugs. This service is accessible anytime and anywhere, with updates available daily or weekly. Use the "Set Alert" function to stay informed. Click on the image below to embark on a brand new journey of drug discovery!
Hiro LS Researcher
The AI Search Engine Built to Accelerate Biopharma Decisions
Search across billion-scale life sciences data to uncover signals, validate evidence, and act with confidence.
Ask any biopharma research question→
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, Patsnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Discover Synapse Data Servers
Synapse data is now integrated into the PatSnap LS Model Context Protocol (MCP) service. Customize your LLM agent now using our MCP server!