Request Demo
What is Plasmin used for?
17 June 2024
Plasmin is a serine protease that plays a crucial role in the body's ability to break down blood clots, a process known as fibrinolysis. This enzyme is derived from plasminogen, an inactive precursor that circulates in the bloodstream. Plasmin is not marketed under any specific drug trade names because it is typically used in its functional form in medical settings rather than as a commercial drug. Its main target is fibrin, the protein that forms the mesh structure of blood clots.
Research institutions around the world are actively studying plasmin, given its potential to treat conditions related to thrombosis, such as myocardial infarction (heart attack), pulmonary embolism, and deep vein thrombosis. Plasmin's role in fibrinolysis makes it a valuable candidate for therapeutic applications aimed at dissolving pathological blood clots that can lead to life-threatening conditions. The enzyme also has implications in cancer research, wound healing, and tissue remodeling, indicating its broad therapeutic potential.
The mechanism of action for plasmin is fundamentally enzymatic. As a serine protease, plasmin cleaves peptide bonds in specific sites within the fibrin mesh that forms the structural backbone of blood clots. When plasminogen is activated to plasmin, either by tissue plasminogen activator (tPA) or urokinase, it targets the fibrin in the clot, leading to the degradation of the polymer into soluble fragments. This breakdown process, known as fibrinolysis, is essential for maintaining vascular health and ensuring that clots are removed once their purpose of stopping bleeding has been fulfilled.
Plasminogen activation can occur naturally within the body, but in medical settings, recombinant tissue plasminogen activator (rtPA) is often administered to expedite this process, particularly in acute settings like ischemic strokes or heart attacks. The timely conversion of plasminogen to plasmin is critical for the effective dissolution of clots that obstruct blood flow to vital tissues.
The administration methods for plasmin or its activators vary depending on the clinical scenario. In emergency settings, such as acute myocardial infarction or ischemic stroke, intravenous administration is the most common route. The onset of action for intravenous administration is typically rapid, occurring within minutes to an hour, which is crucial for minimizing tissue damage due to prolonged lack of blood flow.
For other conditions, such as chronic deep vein thrombosis, plasminogen activators might be delivered through catheters directly to the site of the clot, a procedure known as catheter-directed thrombolysis. This localized approach can be more effective for large, obstructive clots and may reduce systemic side effects.
While plasmin and its activators are generally effective in clot dissolution, they are not without potential side effects. The most significant risk associated with these agents is bleeding, which can range from minor bruising to severe, life-threatening hemorrhages. This risk is partly due to the systemic activation of plasmin, which can degrade fibrin in both pathological and physiological clots, including those protecting the gastrointestinal tract or sites of surgical wounds.
Contraindications for the use of plasminogen activators include active internal bleeding, recent surgery, history of hemorrhagic stroke, and severe uncontrolled hypertension. Patients with these conditions are at elevated risk for catastrophic bleeding events if treated with plasminogen activators.
Patients may also experience hypersensitivity reactions to recombinant proteins, including rtPA. Such reactions can manifest as rash, fever, or more severe anaphylactic responses. Given these risks, the use of plasminogen activators must be carefully weighed against potential benefits, and close monitoring is essential during and after administration.
Other drugs can influence the activity and efficacy of plasmin. Anticoagulants, such as heparin and warfarin, may augment the effects of plasminogen activators by inhibiting the formation of new clots, thereby enhancing the fibrinolytic process. However, this combination also significantly raises the risk of bleeding and must be managed with vigilant monitoring and dosage adjustments.
Nonsteroidal anti-inflammatory drugs (NSAIDs) like aspirin and ibuprofen, which inhibit platelet function, can similarly increase bleeding risk when used concomitantly with plasminogen activators. These medications should be used cautiously, if at all, in patients receiving fibrinolytic therapy.
Conversely, antifibrinolytic agents such as tranexamic acid and aminocaproic acid work by inhibiting plasminogen activation or by directly inhibiting plasmin activity. These agents are often used to treat or prevent excessive bleeding and can counteract the effects of plasminogen activators. Therefore, they should not be used concurrently unless under specific medical guidance for controlling bleeding complications.
In conclusion, plasmin is a pivotal enzyme in the body's fibrinolytic system, responsible for breaking down blood clots and maintaining vascular health. While it holds significant therapeutic promise, especially in acute settings such as heart attacks and strokes, careful consideration of administration methods, potential side effects, and drug interactions is crucial for optimizing patient outcomes and minimizing risks. Ongoing research continues to unravel the full potential of plasmin in various medical fields, promising new advancements in treatment strategies for thrombotic diseases and beyond.
Research institutions around the world are actively studying plasmin, given its potential to treat conditions related to thrombosis, such as myocardial infarction (heart attack), pulmonary embolism, and deep vein thrombosis. Plasmin's role in fibrinolysis makes it a valuable candidate for therapeutic applications aimed at dissolving pathological blood clots that can lead to life-threatening conditions. The enzyme also has implications in cancer research, wound healing, and tissue remodeling, indicating its broad therapeutic potential.
The mechanism of action for plasmin is fundamentally enzymatic. As a serine protease, plasmin cleaves peptide bonds in specific sites within the fibrin mesh that forms the structural backbone of blood clots. When plasminogen is activated to plasmin, either by tissue plasminogen activator (tPA) or urokinase, it targets the fibrin in the clot, leading to the degradation of the polymer into soluble fragments. This breakdown process, known as fibrinolysis, is essential for maintaining vascular health and ensuring that clots are removed once their purpose of stopping bleeding has been fulfilled.
Plasminogen activation can occur naturally within the body, but in medical settings, recombinant tissue plasminogen activator (rtPA) is often administered to expedite this process, particularly in acute settings like ischemic strokes or heart attacks. The timely conversion of plasminogen to plasmin is critical for the effective dissolution of clots that obstruct blood flow to vital tissues.
The administration methods for plasmin or its activators vary depending on the clinical scenario. In emergency settings, such as acute myocardial infarction or ischemic stroke, intravenous administration is the most common route. The onset of action for intravenous administration is typically rapid, occurring within minutes to an hour, which is crucial for minimizing tissue damage due to prolonged lack of blood flow.
For other conditions, such as chronic deep vein thrombosis, plasminogen activators might be delivered through catheters directly to the site of the clot, a procedure known as catheter-directed thrombolysis. This localized approach can be more effective for large, obstructive clots and may reduce systemic side effects.
While plasmin and its activators are generally effective in clot dissolution, they are not without potential side effects. The most significant risk associated with these agents is bleeding, which can range from minor bruising to severe, life-threatening hemorrhages. This risk is partly due to the systemic activation of plasmin, which can degrade fibrin in both pathological and physiological clots, including those protecting the gastrointestinal tract or sites of surgical wounds.
Contraindications for the use of plasminogen activators include active internal bleeding, recent surgery, history of hemorrhagic stroke, and severe uncontrolled hypertension. Patients with these conditions are at elevated risk for catastrophic bleeding events if treated with plasminogen activators.
Patients may also experience hypersensitivity reactions to recombinant proteins, including rtPA. Such reactions can manifest as rash, fever, or more severe anaphylactic responses. Given these risks, the use of plasminogen activators must be carefully weighed against potential benefits, and close monitoring is essential during and after administration.
Other drugs can influence the activity and efficacy of plasmin. Anticoagulants, such as heparin and warfarin, may augment the effects of plasminogen activators by inhibiting the formation of new clots, thereby enhancing the fibrinolytic process. However, this combination also significantly raises the risk of bleeding and must be managed with vigilant monitoring and dosage adjustments.
Nonsteroidal anti-inflammatory drugs (NSAIDs) like aspirin and ibuprofen, which inhibit platelet function, can similarly increase bleeding risk when used concomitantly with plasminogen activators. These medications should be used cautiously, if at all, in patients receiving fibrinolytic therapy.
Conversely, antifibrinolytic agents such as tranexamic acid and aminocaproic acid work by inhibiting plasminogen activation or by directly inhibiting plasmin activity. These agents are often used to treat or prevent excessive bleeding and can counteract the effects of plasminogen activators. Therefore, they should not be used concurrently unless under specific medical guidance for controlling bleeding complications.
In conclusion, plasmin is a pivotal enzyme in the body's fibrinolytic system, responsible for breaking down blood clots and maintaining vascular health. While it holds significant therapeutic promise, especially in acute settings such as heart attacks and strokes, careful consideration of administration methods, potential side effects, and drug interactions is crucial for optimizing patient outcomes and minimizing risks. Ongoing research continues to unravel the full potential of plasmin in various medical fields, promising new advancements in treatment strategies for thrombotic diseases and beyond.
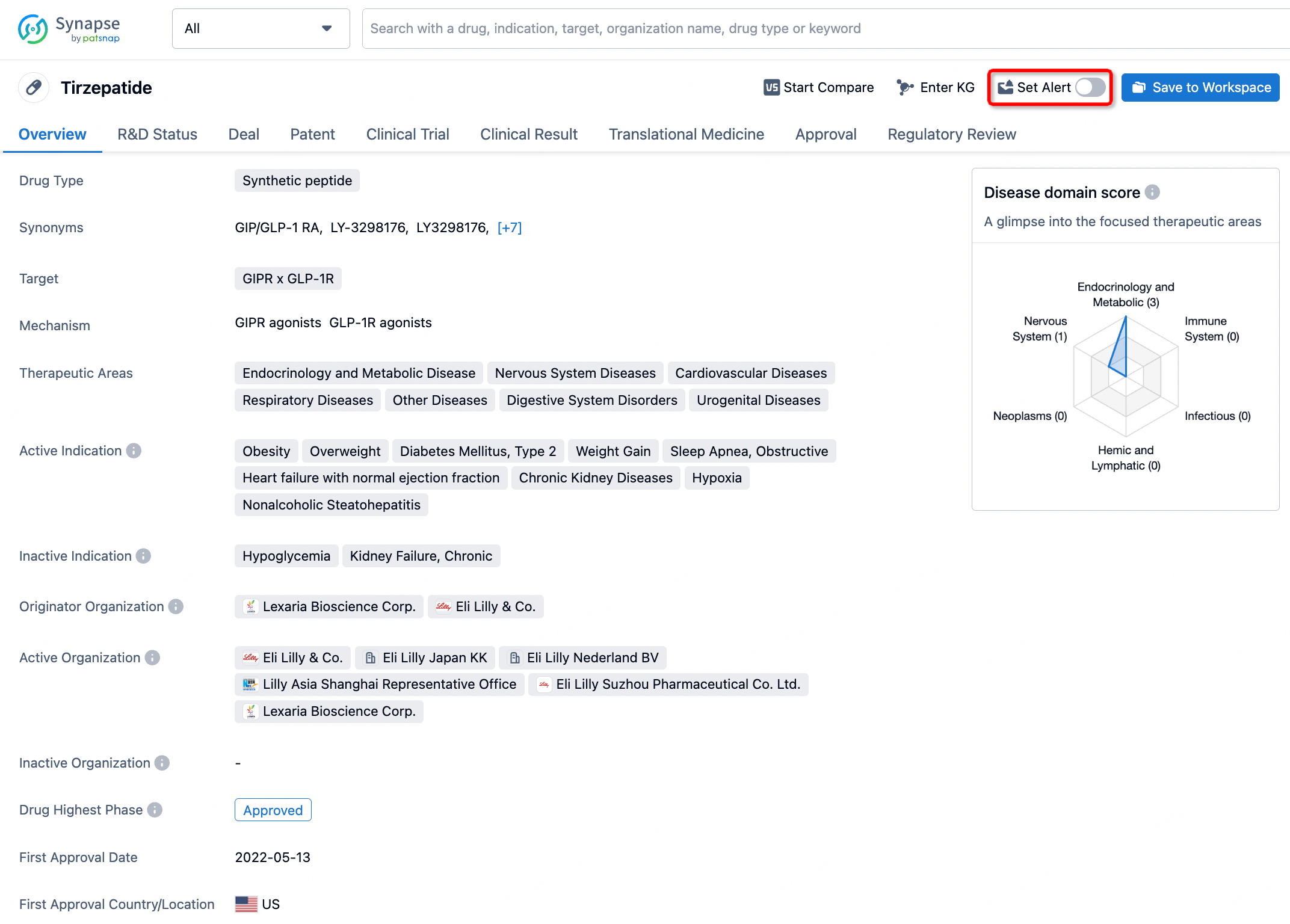
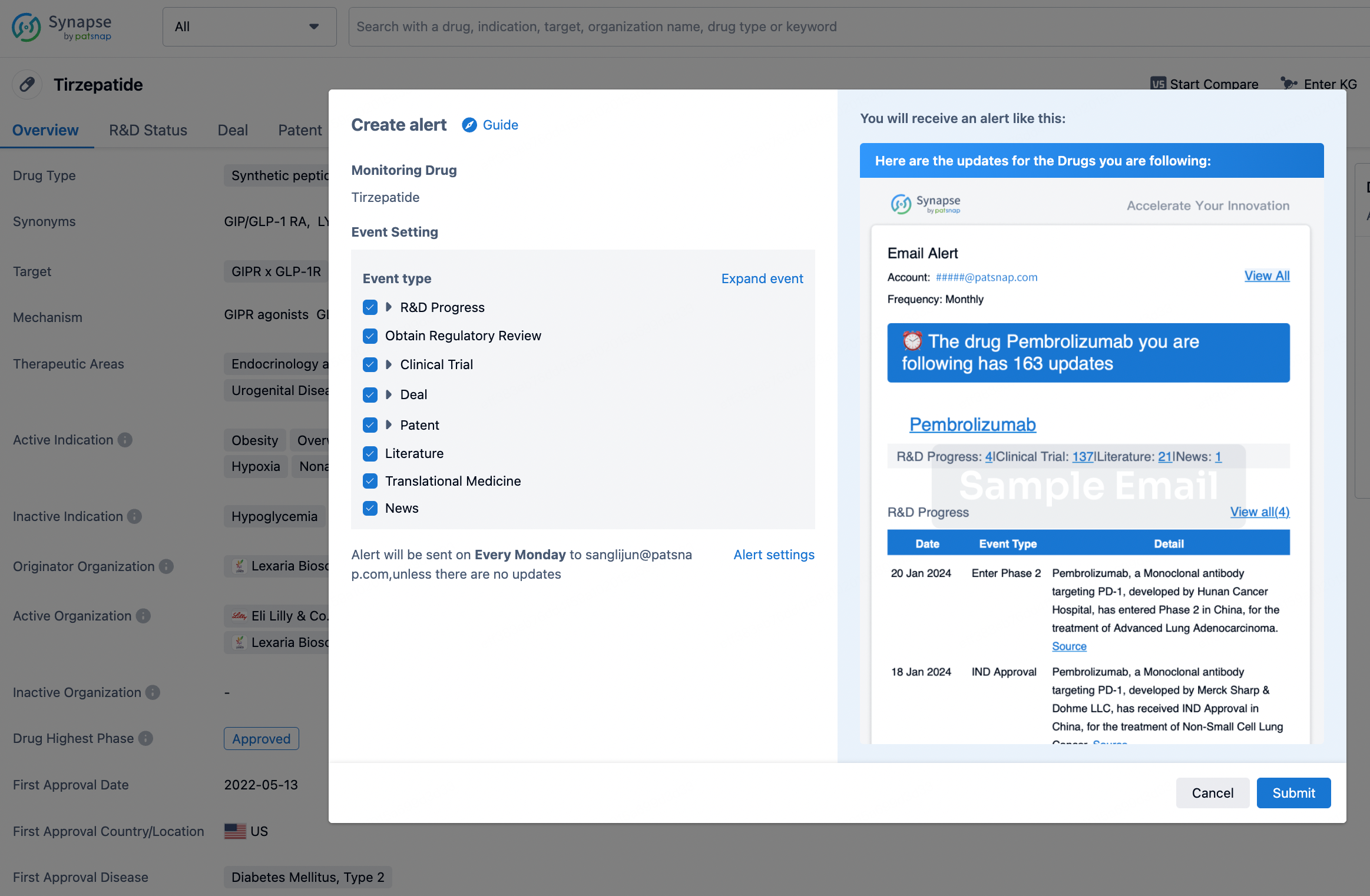
How to obtain the latest development progress of all drugs?
In the Synapse database, you can stay updated on the latest research and development advances of all drugs. This service is accessible anytime and anywhere, with updates available daily or weekly. Use the "Set Alert" function to stay informed. Click on the image below to embark on a brand new journey of drug discovery!
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.