Request Demo
Last update 17 Jun 2026
Clarithromycin
Last update 17 Jun 2026
Overview
Basic Info
Drug Type Small molecule drug |
Synonyms 6-O-methyl erythromycin, 6-O-methylerythromycin, 6-O-methylerythromycin A + [89] |
Target |
Action inhibitors |
Mechanism 50S subunit inhibitors(50S ribosomal subunit inhibitors) |
Therapeutic Areas |
Active Indication |
Inactive Indication |
Originator Organization |
Active Organization |
Inactive Organization |
License Organization- |
Drug Highest PhaseApproved |
First Approval Date- |
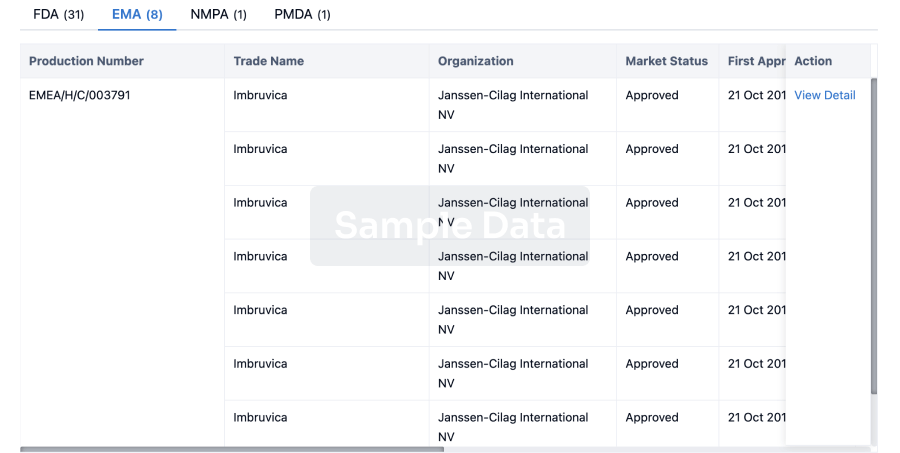
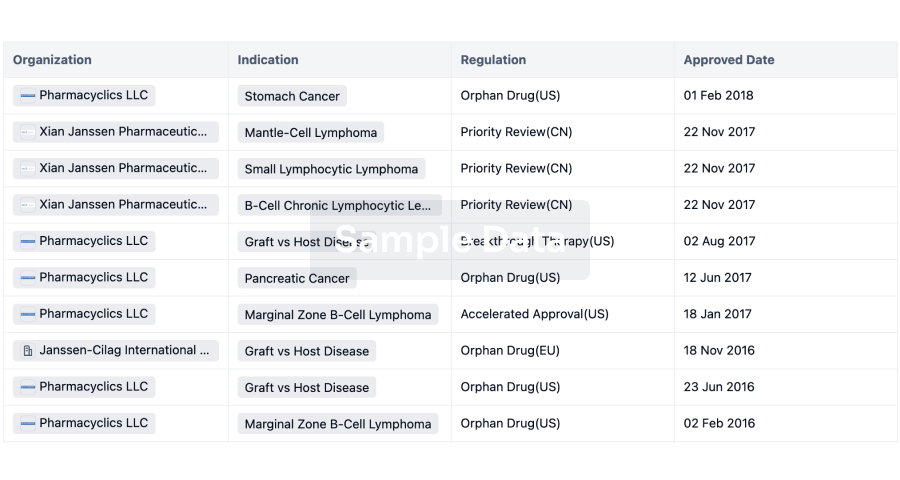
RegulationAccelerated Approval (United States), Priority Review (China), Orphan Drug (Japan) |



Login to view timeline
Structure/Sequence
Molecular FormulaC38H69NO13 |
InChIKeyAGOYDEPGAOXOCK-KCBOHYOISA-N |
CAS Registry81103-11-9 |
Related
508
Clinical Trials associated with ClarithromycinNCT07485010
A Multi-centre, Randomised Trial Comparing a Novel Combination Treatment (Arm D - Intravenous Sulbactam-durlobactam in Combination With Intravenous Ceftriaxone, Oral Amoxicillin, Oral Azithromycin and Oral Clofazimine) Versus Standard of Care Treatments for the Intensive Phase of Treatment for Mycobacterium Abscessus Pulmonary Disease in People With or Without Cystic Fibrosis in the Finding the Optimal Regimen for Mycobacterium Abscessus Treatment (FORMaT) Adaptive Platform Trial

NCT07439445
Efficacy and Safety of Simplified Regimen Guided by Fecal Clarithromycin Resistance Gene Detection for First-line Helicobacter Pylori Eradication
ChiCTR2600122928
Keverprazan combined with different doses of amoxicillin dual therapy for first-line Helicobacter pylori eradication: a prospective, randomized controlled trial
100 Clinical Results associated with Clarithromycin
Login to view more data
100 Translational Medicine associated with Clarithromycin
Login to view more data
100 Patents (Medical) associated with Clarithromycin
Login to view more data
12,357
Literatures (Medical) associated with Clarithromycin31 Dec 2026ANNALS OF MEDICINE
Comparative evaluation of molecular technologies for the identification of prevalent non-tuberculous mycobacteria in pulmonary infections: a systematic review and meta-analysis
Review
Author: Molicotti, Paola ; Sechi, Leonardo Antonio ; You, Yanshan ; Chen, Xiang ; Sun, Jiawen ; Chen, Xibin
BACKGROUND:
The increasing prevalence of non-tuberculous mycobacteria pulmonary disease (NTM PD) is a burden to public health. Successful management of NTM PD critically depends on accurate species identification and reliable drug susceptibility testing to guide appropriate antibiotic therapy. Emerging molecular technologies offer rapid diagnostic solutions compared to conventional methods, but their performance varies. This study aims to provide a comprehensive evaluation of current molecular techniques for NTM identification and to present a global antibiotic resistance profile.
METHODS:
A systematic literature search was conducted in PubMed and Web of Science for studies published between 2005 and 2024. Studies applying molecular methods for NTM identification and resistance detection in humans were included. Data on study characteristics, diagnostic methods, sample types, sample sizes, identification sensitivity, and drug susceptibility results were extracted. Meta-analysis was performed using R with the meta4diag package. The quality of included studies was assessed using the QUADAS-2 tool.
RESULTS:
The analysis included 49 studies on NTM identification and 33 studies on antibiotic resistance. For species identification, all evaluated molecular technologies (MALDI-TOF MS, PCR-based methods, Sequencing, DNA chip, and DNA strip) demonstrated high pooled sensitivities (>0.92). Subgroup analysis revealed that sample type significantly affected performance for MALDI-TOF MS. Preliminary analysis of antibiotic resistance rates revealed varying patterns. For slowly growing mycobacteria, a significantly high Ethambutol resistance rate was observed in M. avium (69.20%). Among rapidly growing mycobacteria, resistance to Imipenem was notable (54.22%), and Clarithromycin resistance varied significantly within the Mycobacterium abscessus complex.
CONCLUSION:
Emerging molecular technologies have revolutionized the methodology for NTM identification with excellent performance. However, their performance can be influenced by sample type, particularly for MALDI-TOF MS. The alarming and heterogeneous antibiotic resistance patterns also highlight the critical need for rapid and accurate species identification and drug susceptibility testing to inform effective therapeutic strategies. Key messagesMolecular technologies demonstrate high accuracy for NTM identification.Antibiotic resistance is a serious concern with variations among NTM species and subspecies.Rapid and accurate species identification and drug susceptibility testing are crucial for guiding effective clinical management of NTM PD.
01 Dec 2026MOLECULAR BIOLOGY REPORTS
Impact of clarithromycin on monocytes-macrophages in patients with coronary arterial disease: a crucial study in cardiovascular research
Article
Author: Cruz-González, Daniela de Jesus ; Martínez-Shio, Elena Berenice ; Marín-Jáuregui, Laura Sherell ; Escobedo-Uribe, Carlos David ; Monsiváis-Urenda, Adriana Elizabeth
01 Oct 2026TISSUE & CELL
Vitamin D3 in synergy with triple therapy to eradicate Helicobacter pylori infection in mice via the c-Raf/MEK/ERK pathway
Article
Author: Xin, Yi ; Zhao, Shuai ; Wang, Wenxiao ; Shan, Chengyan ; Zhong, Yaoyao ; Wan, Daihong
BACKGROUND:
Helicobacter pylori (H. pylori) is a primary pathogen associated with gastritis, peptic ulcers, and gastric cancer. Current eradication therapies are increasingly compromised by antibiotic resistance. Vitamin D3 (VD3) has shown potential as an adjunct therapy, yet its underlying mechanism remains unclear.
OBJECTIVE:
This study evaluated the efficacy of VD3 combined with triple therapy on H. pylori eradication in mice, assessing pathological changes, infection and inflammation levels and epithelial cell death; furthermore, it explored the mechanism of the synergistic effect.
METHODS:
An in vivo model was inoculated with H. pylori to establish in mice. After four weeks, mice were treated with VD3, triple therapy, quadruple therapy (omeprazole, amoxicillin, clarithromycin and bismuth potassium citrate), or their combinations for another four weeks. Hematoxylin and Eosin (H&E) staining, quantitative real-time PCR, colony formation, immunoblotting, enzyme-linked immunosorbent assay (ELISA), TUNEL staining, and caspase activity assays were used to evaluate the effect of VD3.
RESULTS:
Compared to triple therapy alone, the combination of VD3 and triple therapy reduced gastritis severity, H. pylori 16S rDNA expression, and bacterial colony counts in infected mice. It also decreased mRNA and protein levels of inflammatory cytokines IL-1β, IL-6, and TNF-α, reduced gastric epithelial cell apoptosis, and suppressed caspase-3/6/9 activities. VD3 treatment further enhanced c-Raf, MEK, and ERK phosphorylation in gastric tissues. Importantly, the ERK inhibitor U0126 abrogated the therapeutic benefits of VD3 combined with triple therapy, leading to increased gastritis severity, H. pylori 16S rDNA expression, bacterial colony counts, and caspase activity.
CONCLUSION:
Vitamin D3 synergizes with triple therapy to eradicate H. pylori infection by exhibiting antibacterial, anti-inflammatory, and cytoprotective effects through regulation of the c-Raf/MEK/ERK signaling pathway.
209
News (Medical) associated with Clarithromycin22 May 2026
20 May 2026
Clinical ResultPhase 3Drug ApprovalPhase 1
100 Deals associated with Clarithromycin
Login to view more data
External Link
| KEGG | Wiki | ATC | Drug Bank |
|---|---|---|---|
| D00276 | Clarithromycin |
R&D Status
Approved
10 top approved records. to view more data
Login
| Indication | Country/Location | Organization | Date |
|---|---|---|---|
| Group a Streptococcal Pharyngitis | Australia | 05 May 2026 | |
| Peptic Ulcer | Australia | 05 May 2026 | |
| Mycobacterium Avium-Intracellulare Infection | Japan | 06 Oct 2009 | |
| Scarlet Fever | Japan | 15 Mar 2006 | |
| Secondary infection | Japan | 15 Mar 2006 | |
| Community Acquired Pneumonia | United States | 03 Mar 2000 | |
| Lower Respiratory Tract Infections | China | 01 Jan 1996 | |
| Lower Respiratory Tract Infections | China | 01 Jan 1996 | |
| Acute maxillary sinusitis | United States | 31 Oct 1991 | |
| Acute otitis media | United States | 31 Oct 1991 | |
| Bronchitis, Chronic | United States | 31 Oct 1991 | |
| Duodenal Ulcer | United States | 31 Oct 1991 | |
| Helicobacter pylori infection | United States | 31 Oct 1991 | |
| HIV Infections | United States | 31 Oct 1991 | |
| Infectious Diseases | United States | 31 Oct 1991 | |
| Mycobacterium Infections | United States | 31 Oct 1991 | |
| Mycobacterium Infections, Nontuberculous | United States | 31 Oct 1991 | |
| Rheumatic Fever | United States | 31 Oct 1991 | |
| Abscess | Japan | 29 Mar 1991 | |
| Acute Bronchitis | Japan | 29 Mar 1991 |

Developing
10 top R&D records. to view more data
Login
| Indication | Highest Phase | Country/Location | Organization | Date |
|---|---|---|---|---|
| Gram-negative bacteremia | Phase 3 | Belgium | 15 Dec 2017 | |
| Gram-negative bacteremia | Phase 3 | Greece | 15 Dec 2017 | |
| Gram-Negative Bacterial Infections | Phase 3 | Belgium | 15 Dec 2017 | |
| Gram-Negative Bacterial Infections | Phase 3 | Greece | 15 Dec 2017 | |
| Hospital-acquired pneumonia | Phase 3 | Belgium | 15 Dec 2017 | |
| Hospital-acquired pneumonia | Phase 3 | Greece | 15 Dec 2017 | |
| Pneumonia, Ventilator-Associated | Phase 3 | Belgium | 15 Dec 2017 | |
| Pneumonia, Ventilator-Associated | Phase 3 | Greece | 15 Dec 2017 | |
| Respiratory Distress Syndrome | Phase 3 | Belgium | 15 Dec 2017 | |
| Respiratory Distress Syndrome | Phase 3 | Greece | 15 Dec 2017 |

Login to view more data
Clinical Result
Clinical Result
Indication
Phase
Evaluation
View All Results
Phase 1/2 | 28 | rkwwjnrkyt(gtkoyrgdrt) = vosiqsttjw glomeuscfe (erejmpscau ) View more | Positive | 01 Aug 2025 | |||
Phase 3 | Community Acquired Pneumonia procalcitonin | 267 | Standard of care + Clarithromycin | pprogrvqmm(wiolsjxwhi) = wvydvgxdbj yhhufajnuy (bxtedfrqqs ) View more | Positive | 01 Jan 2024 | |
Standard of care + placebo | pprogrvqmm(wiolsjxwhi) = oyningbpux yhhufajnuy (bxtedfrqqs ) View more | ||||||
Phase 3 | 12 | (BiRD Treatment Regimen) | yuvzmhapzb(xhyctjzukz) = jbgylngszw gxgfxssery (qclhitkhpy, eviehomtdo - xjdzjfeyib) View more | - | 05 Jun 2023 | ||
(Rd Treatment Regimen) | yuvzmhapzb(xhyctjzukz) = bgddnrrcpi gxgfxssery (qclhitkhpy, zsclebzegq - jqgovzxodn) View more | ||||||
Early Phase 1 | - | 92 | Placebo (Water) | fvoxcrosvk(rlpfhqrtat) = jghlpznmpl uedbyqqqgf (alwmoghqpr, klnnaajjdm - novmpyaiih) View more | - | 19 Apr 2023 | |
(Rifampin) | fvoxcrosvk(rlpfhqrtat) = ziypxocytq uedbyqqqgf (alwmoghqpr, kodurhtokk - qurrcmgxxh) View more | ||||||
Phase 4 | 112 | (High Dose Dual Therapy) | iqppvwpmdx = xowygfnqzn qozmshlpvm (hzjkajrcxh, xmuaqvisuq - viywkfqeut) View more | - | 01 Feb 2023 | ||
(Standard Triple Therapy) | iqppvwpmdx = uuefpscuia qozmshlpvm (hzjkajrcxh, bnemoylauo - lkuzarpeut) View more | ||||||
Phase 1/2 | 34 | (Transdermal Flumazenil (Active)) | aeipsradxn(fhotnmzwev) = dyybyqlwfz vwonlfstpz (bdplqxsxax, wyndznwvpn - xxnwrnhmbj) View more | - | 10 Jan 2023 | ||
Placebo (Placebo Cream) | aeipsradxn(fhotnmzwev) = ymdoqudznc vwonlfstpz (bdplqxsxax, htwxqyrdlw - xfdwxkszur) View more | ||||||
Phase 3 | 110 | oigvkotdnn(rqmtewujiq) = fjohrkxasm ztvhnncqge (zwyrnkrzhv ) | Negative | 18 Jun 2022 | |||
Placebo | oigvkotdnn(rqmtewujiq) = kmdeenqtqq ztvhnncqge (zwyrnkrzhv ) | ||||||
Phase 1/2 | 32 | tsluphfmes(hasngzykzu) = swzapxnfer tiiwgapkxp (rezbuetgbq ) View more | - | 08 Sep 2021 | |||
Phase 2 | 90 | Oral Clarithromycin | xvyjjridwk(juaqvzhgfy) = vdmgthkdvy pjsgpnmvdu (pknuzdsbid, 78.1 - 92.2) | Positive | 06 Aug 2021 | ||
Phase 3 | 286 | ewgaxcmevp(zxqopaoqka) = raqsgoymze aiwfzyzpnj (egsgisutcn ) View more | Negative | 21 May 2021 | |||
Lenalidomide+dexamethasone | ewgaxcmevp(zxqopaoqka) = xvblzatygd aiwfzyzpnj (egsgisutcn ) View more |

Login to view more data
Translational Medicine
Boost your research with our translational medicine data.
login
or

Deal
Boost your decision using our deal data.
login
or

Core Patent
Boost your research with our Core Patent data.
login
or

Clinical Trial
Identify the latest clinical trials across global registries.
login
or

Approval
Accelerate your research with the latest regulatory approval information.
login
or
Regulation
Understand key drug designations in just a few clicks with Synapse.
login
or
Hiro LS Researcher
The AI Search Engine Built to Accelerate Biopharma Decisions
Search across billion-scale life sciences data to uncover signals, validate evidence, and act with confidence.
Ask any biopharma research question→
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, Patsnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Discover Synapse Data Servers
Synapse data is now integrated into the PatSnap LS Model Context Protocol (MCP) service. Customize your LLM agent now using our MCP server!
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free