Request Demo
What is Irinotecan Hydrochloride used for?
14 June 2024
Irinotecan Hydrochloride is a chemotherapy agent commonly referred to under trade names such as Camptosar, Campto, and CPT-11. This drug is primarily used for the treatment of metastatic colorectal cancer, but has also found applications in treating other malignancies, including small cell lung cancer and pancreatic cancer. The development and research related to Irinotecan Hydrochloride have seen contributions from numerous research institutions around the globe, with significant advances being made in oncology research laboratories. As a derivative of camptothecin, a natural alkaloid extracted from the Chinese tree Camptotheca acuminata, Irinotecan belongs to a class of drugs known as topoisomerase inhibitors. This category of chemotherapy drugs functions by interfering with the DNA replication process in cancer cells, thereby inhibiting their growth and proliferation.
The mechanism of action of Irinotecan Hydrochloride is complex yet fascinating. It primarily targets and inhibits the enzyme topoisomerase I. This enzyme plays a critical role in DNA replication by creating transient single-strand breaks in the DNA structure to relieve torsional strain during the unwinding of the double helix. Irinotecan stabilizes the complex formed between topoisomerase I and DNA, preventing the re-ligation or repair of these single-strand breaks. As a result, the accumulation of these breaks eventually leads to double-strand breaks during DNA synthesis, which is catastrophic for the cancer cells, causing cell death. Furthermore, Irinotecan is a prodrug, meaning it requires conversion to its active form, SN-38, by liver carboxylesterases to exert its anticancer effects. SN-38 is significantly more potent than the parent compound and is responsible for much of Irinotecan's efficacy as a chemotherapeutic agent.
Irinotecan Hydrochloride can be administered through intravenous infusion, typically over a period of 90 minutes. The administration schedule can vary based on the specific cancer being treated, the regimen being followed, and the patient's overall health and response to treatment. Commonly, it is given once every two weeks or once a week, but the frequency and dosage can be adjusted by the oncologist based on individual patient factors. After administration, the onset of action generally occurs within a few hours, but the therapeutic effects, including tumor response, may take weeks to become evident. To maximize efficacy and minimize side effects, careful monitoring and adjustments are essential throughout the treatment cycle.
Despite its effectiveness, Irinotecan Hydrochloride is associated with several side effects, which can range from mild to severe. The most common side effect is diarrhea, which can be acute (occurring within 24 hours of infusion) or delayed (occurring more than 24 hours after infusion). Acute diarrhea is often accompanied by symptoms such as abdominal cramping and can be managed with atropine. Delayed diarrhea, however, can be severe and necessitates prompt treatment with loperamide and hydration to prevent dehydration. Another significant side effect is myelosuppression, which includes neutropenia, anemia, and thrombocytopenia. Patients undergoing treatment with Irinotecan require regular blood tests to monitor these levels and prevent complications. Other side effects may include nausea, vomiting, fatigue, hair loss, and mouth sores. There are several contraindications for Irinotecan use, including known hypersensitivity to the drug, severe bone marrow suppression, and certain genetic conditions like Gilbert's syndrome, which can affect drug metabolism and increase toxicity.
The interaction of Irinotecan Hydrochloride with other drugs is an essential consideration for both oncologists and patients. Several drugs can affect the metabolism and efficacy of Irinotecan. For example, enzyme-inducing anticonvulsants like phenytoin, carbamazepine, and phenobarbital can increase the metabolism of Irinotecan, potentially reducing its effectiveness. Conversely, drugs that inhibit the enzyme CYP3A4, such as ketoconazole, can increase the levels of Irinotecan and its active metabolite SN-38, raising the risk of toxicity. Co-administration with other chemotherapeutic agents, such as fluorouracil and leucovorin, is common practice in treating colorectal cancer, but this combination requires careful dose adjustments and monitoring due to the increased risk of side effects. Additionally, anticoagulants such as warfarin may interact with Irinotecan, necessitating more frequent monitoring of blood clotting parameters to prevent either excessive bleeding or clot formation.
In conclusion, Irinotecan Hydrochloride is a potent chemotherapeutic agent with a unique mechanism of action targeting topoisomerase I. Its administration requires careful consideration of dosing schedules, potential side effects, and drug interactions to maximize its therapeutic benefits while minimizing risks. Ongoing research and clinical trials continue to refine its use and explore new therapeutic combinations, aiming to improve outcomes for patients battling various forms of cancer. As with any chemotherapy treatment, the management of Irinotecan therapy necessitates a collaborative approach between the patient and their healthcare team to navigate the complexities of cancer treatment effectively.
The mechanism of action of Irinotecan Hydrochloride is complex yet fascinating. It primarily targets and inhibits the enzyme topoisomerase I. This enzyme plays a critical role in DNA replication by creating transient single-strand breaks in the DNA structure to relieve torsional strain during the unwinding of the double helix. Irinotecan stabilizes the complex formed between topoisomerase I and DNA, preventing the re-ligation or repair of these single-strand breaks. As a result, the accumulation of these breaks eventually leads to double-strand breaks during DNA synthesis, which is catastrophic for the cancer cells, causing cell death. Furthermore, Irinotecan is a prodrug, meaning it requires conversion to its active form, SN-38, by liver carboxylesterases to exert its anticancer effects. SN-38 is significantly more potent than the parent compound and is responsible for much of Irinotecan's efficacy as a chemotherapeutic agent.
Irinotecan Hydrochloride can be administered through intravenous infusion, typically over a period of 90 minutes. The administration schedule can vary based on the specific cancer being treated, the regimen being followed, and the patient's overall health and response to treatment. Commonly, it is given once every two weeks or once a week, but the frequency and dosage can be adjusted by the oncologist based on individual patient factors. After administration, the onset of action generally occurs within a few hours, but the therapeutic effects, including tumor response, may take weeks to become evident. To maximize efficacy and minimize side effects, careful monitoring and adjustments are essential throughout the treatment cycle.
Despite its effectiveness, Irinotecan Hydrochloride is associated with several side effects, which can range from mild to severe. The most common side effect is diarrhea, which can be acute (occurring within 24 hours of infusion) or delayed (occurring more than 24 hours after infusion). Acute diarrhea is often accompanied by symptoms such as abdominal cramping and can be managed with atropine. Delayed diarrhea, however, can be severe and necessitates prompt treatment with loperamide and hydration to prevent dehydration. Another significant side effect is myelosuppression, which includes neutropenia, anemia, and thrombocytopenia. Patients undergoing treatment with Irinotecan require regular blood tests to monitor these levels and prevent complications. Other side effects may include nausea, vomiting, fatigue, hair loss, and mouth sores. There are several contraindications for Irinotecan use, including known hypersensitivity to the drug, severe bone marrow suppression, and certain genetic conditions like Gilbert's syndrome, which can affect drug metabolism and increase toxicity.
The interaction of Irinotecan Hydrochloride with other drugs is an essential consideration for both oncologists and patients. Several drugs can affect the metabolism and efficacy of Irinotecan. For example, enzyme-inducing anticonvulsants like phenytoin, carbamazepine, and phenobarbital can increase the metabolism of Irinotecan, potentially reducing its effectiveness. Conversely, drugs that inhibit the enzyme CYP3A4, such as ketoconazole, can increase the levels of Irinotecan and its active metabolite SN-38, raising the risk of toxicity. Co-administration with other chemotherapeutic agents, such as fluorouracil and leucovorin, is common practice in treating colorectal cancer, but this combination requires careful dose adjustments and monitoring due to the increased risk of side effects. Additionally, anticoagulants such as warfarin may interact with Irinotecan, necessitating more frequent monitoring of blood clotting parameters to prevent either excessive bleeding or clot formation.
In conclusion, Irinotecan Hydrochloride is a potent chemotherapeutic agent with a unique mechanism of action targeting topoisomerase I. Its administration requires careful consideration of dosing schedules, potential side effects, and drug interactions to maximize its therapeutic benefits while minimizing risks. Ongoing research and clinical trials continue to refine its use and explore new therapeutic combinations, aiming to improve outcomes for patients battling various forms of cancer. As with any chemotherapy treatment, the management of Irinotecan therapy necessitates a collaborative approach between the patient and their healthcare team to navigate the complexities of cancer treatment effectively.
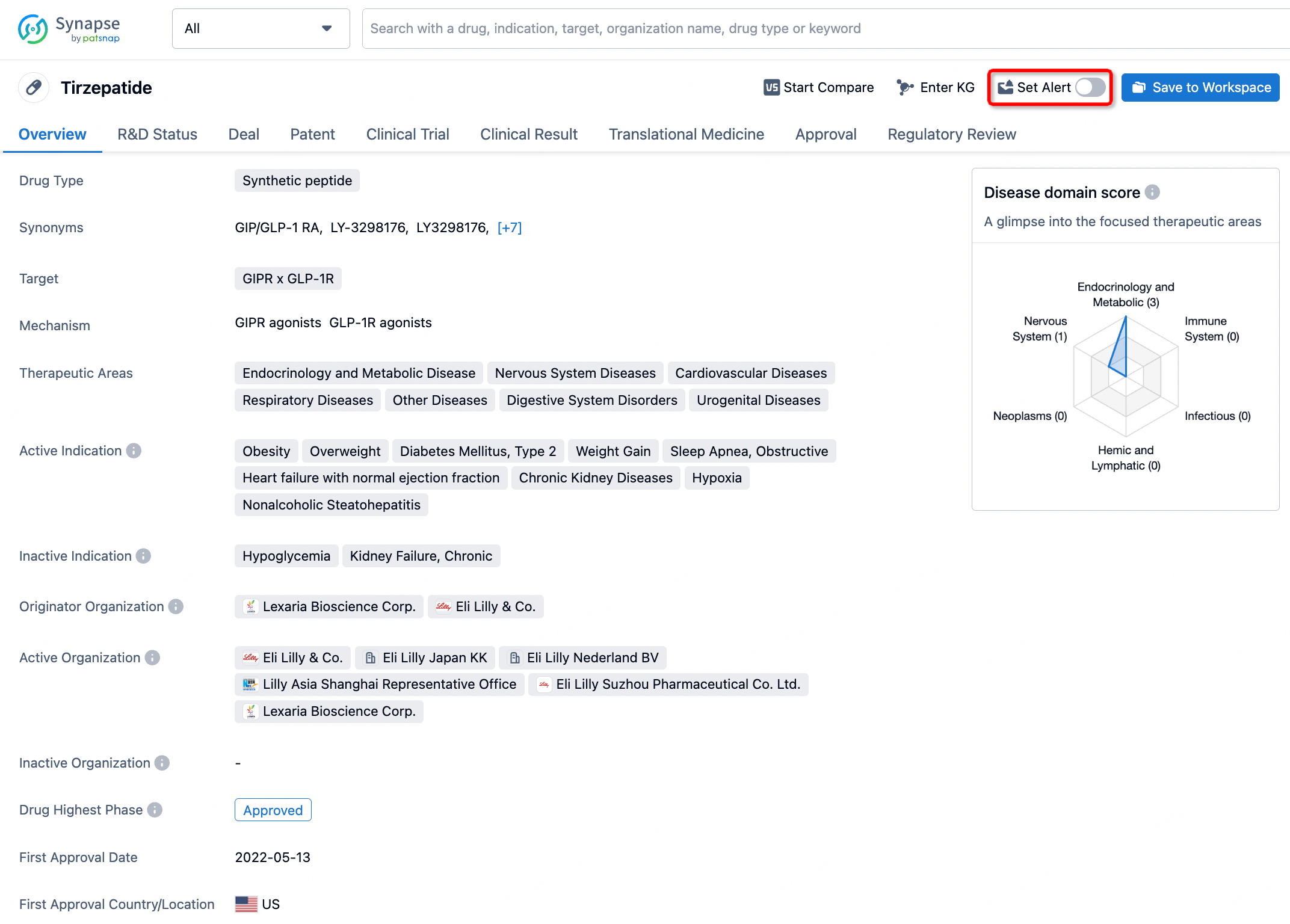
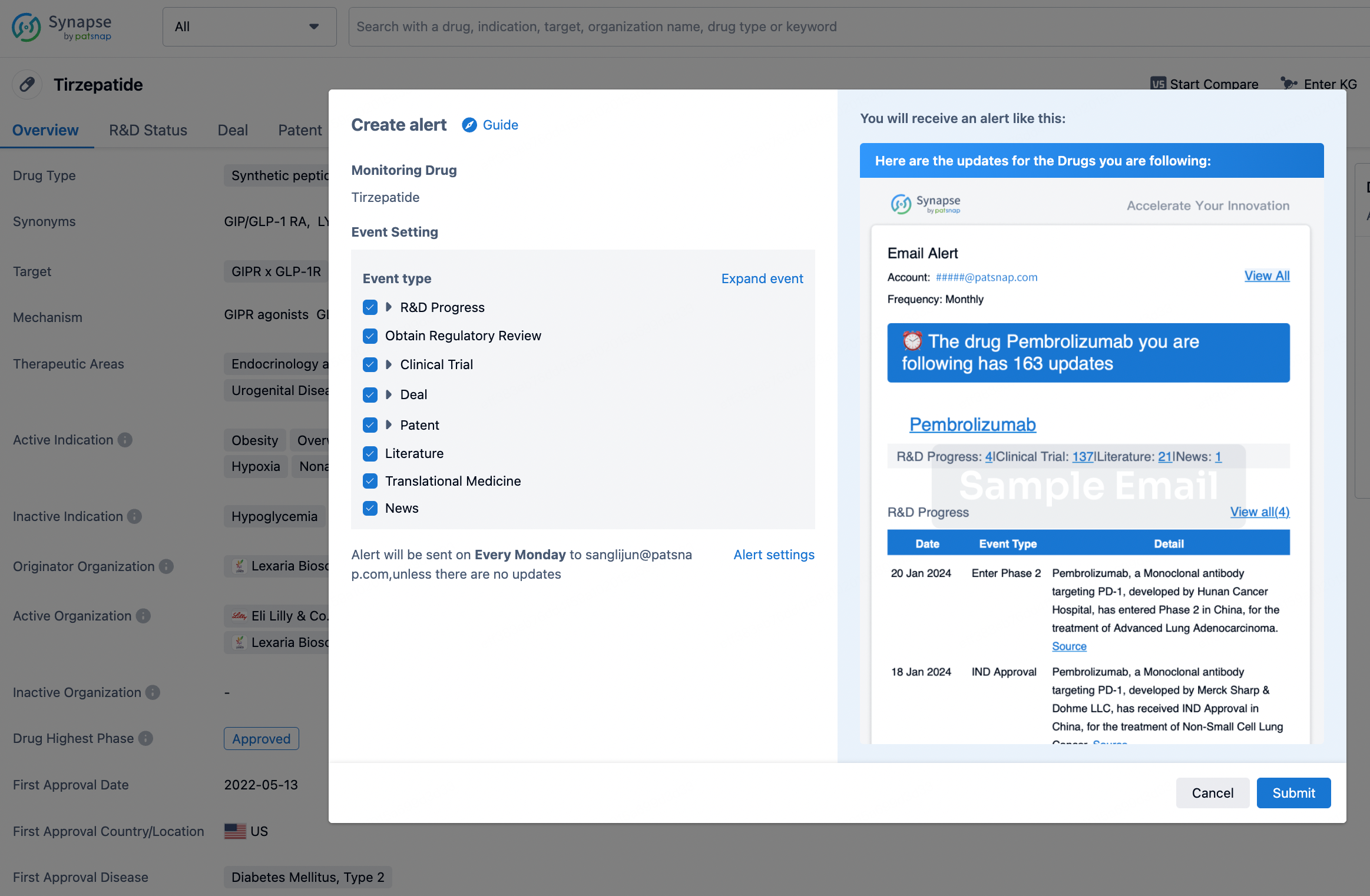
How to obtain the latest development progress of all drugs?
In the Synapse database, you can stay updated on the latest research and development advances of all drugs. This service is accessible anytime and anywhere, with updates available daily or weekly. Use the "Set Alert" function to stay informed. Click on the image below to embark on a brand new journey of drug discovery!
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.