Request Demo
What is Cholecalciferol Chloesterol used for?
15 June 2024
Cholecalciferol, commonly known as vitamin D3, is a vital nutrient that plays a crucial role in maintaining bone health and supporting the immune system. It is widely used in dietary supplements and fortified foods. On the other hand, cholesterol is a lipid molecule that is essential for the formation of cell membranes, hormone production, and other vital bodily functions. While these two compounds serve different purposes in the body, they are interconnected in interesting ways. This blog post delves into the relationship between cholecalciferol and cholesterol, exploring their mechanisms of action, how to use them, potential side effects, and interactions with other drugs.
Cholecalciferol Chloesterol Introduction:
Cholecalciferol, sold under various trade names such as D3-Max, Bio-D-Mulsion, and Calcirol, targets the vitamin D receptors (VDR) in the body. It is primarily used to treat and prevent vitamin D deficiency, which can lead to bone disorders such as rickets in children and osteomalacia in adults. Research institutions across the globe have been investigating the broader implications of vitamin D, including its role in immune function, cardiovascular health, and even cancer prevention. Cholecalciferol is available in various forms, including tablets, capsules, and liquid drops, and can be obtained both over-the-counter and through prescription.
Cholesterol, though often vilified due to its association with cardiovascular disease, is an essential molecule in the body. It serves as a building block for cell membranes, hormones (such as estrogen and testosterone), and bile acids, which aid in fat digestion. Cholesterol is synthesized in the liver and can also be obtained from dietary sources. It is important to distinguish between high-density lipoprotein (HDL) cholesterol, which is considered "good," and low-density lipoprotein (LDL) cholesterol, which is considered "bad" because high levels can lead to plaque buildup in the arteries.
Cholecalciferol Chloesterol Mechanism of Action:
Cholecalciferol is converted in the liver to 25-hydroxyvitamin D (calcidiol), the major circulating form of vitamin D. Calcidiol is then converted in the kidneys to its active form, 1,25-dihydroxyvitamin D (calcitriol). Calcitriol binds to vitamin D receptors (VDR) in various tissues, including the intestines, bones, and kidneys, to regulate calcium and phosphate metabolism. This action is crucial for maintaining healthy bone structure and mineralization.
Cholesterol metabolism is a complex process involving multiple pathways. Cholesterol is synthesized in the liver through a multi-step process that begins with acetyl-CoA and involves the enzyme HMG-CoA reductase, a key regulatory step in cholesterol synthesis. Cholesterol can be transported in the bloodstream by lipoproteins, including HDL and LDL. HDL is responsible for transporting cholesterol from peripheral tissues back to the liver for excretion, a process known as reverse cholesterol transport. In contrast, LDL carries cholesterol to peripheral tissues, where it can be used for cell membrane synthesis and hormone production.
How to Use Cholecalciferol Chloesterol:
Cholecalciferol is typically administered orally in the form of tablets, capsules, or liquid drops. The dosage varies depending on the individual's age, health status, and the severity of vitamin D deficiency. For example, the recommended dietary allowance (RDA) for adults ranges from 600 to 800 IU (international units) per day, while higher doses may be prescribed for individuals with severe deficiency or certain medical conditions. It is generally advised to take cholecalciferol with a meal containing fat to enhance absorption, as vitamin D is fat-soluble.
The onset of action for cholecalciferol can vary. While it may take several days to weeks for serum 25-hydroxyvitamin D levels to rise significantly, the clinical effects on bone health and calcium metabolism may take several months to become apparent. Regular monitoring of vitamin D levels and calcium status is recommended during supplementation to ensure efficacy and safety.
Cholesterol levels can be managed through lifestyle modifications, dietary changes, and medication if necessary. Statins are the most commonly prescribed drugs for lowering LDL cholesterol levels. These medications inhibit HMG-CoA reductase, the enzyme involved in cholesterol synthesis in the liver. Other lipid-lowering agents include bile acid sequestrants, niacin, and fibrates, which target different aspects of cholesterol metabolism.
What is Cholecalciferol Chloesterol Side Effects:
Cholecalciferol is generally well-tolerated when taken at recommended dosages. However, excessive intake can lead to hypervitaminosis D, a condition characterized by elevated levels of vitamin D in the blood. Symptoms of hypervitaminosis D include hypercalcemia (high levels of calcium in the blood), which can cause nausea, vomiting, weakness, frequent urination, and kidney stones. Severe hypercalcemia can lead to more serious complications such as arrhythmias and kidney failure.
Contraindications for cholecalciferol use include hypercalcemia, vitamin D toxicity, and certain conditions such as sarcoidosis and primary hyperparathyroidism, where patients may already have elevated levels of calcium or vitamin D. Individuals with kidney disease should also use cholecalciferol cautiously, as their ability to convert vitamin D to its active form may be impaired.
Cholesterol-lowering medications, particularly statins, can also have side effects. Common side effects of statins include muscle pain, fatigue, and digestive problems. Rare but serious side effects include liver damage, myopathy (muscle disease), and increased risk of type 2 diabetes. Patients on statins should have their liver function monitored regularly.
What Other Drugs Will Affect Cholecalciferol Chloesterol:
Several drugs can interact with cholecalciferol, affecting its absorption, metabolism, or efficacy. For example, corticosteroids can reduce calcium absorption and impair vitamin D metabolism, potentially necessitating higher doses of cholecalciferol. Orlistat, a weight-loss medication, can reduce the absorption of fat-soluble vitamins, including vitamin D. Anticonvulsants such as phenytoin and phenobarbital can increase the metabolism of vitamin D, leading to lower serum levels.
Cholesterol-lowering medications can also interact with other drugs. Statins, for example, are metabolized by the liver enzyme CYP3A4. Drugs that inhibit this enzyme, such as certain antibiotics (e.g., clarithromycin), antifungal agents (e.g., ketoconazole), and grapefruit juice, can increase statin levels in the blood, raising the risk of side effects. Conversely, drugs that induce CYP3A4, such as rifampin, can reduce statin levels and efficacy. Additionally, combining statins with other lipid-lowering agents like fibrates can increase the risk of muscle-related side effects.
In conclusion, cholecalciferol (vitamin D3) and cholesterol play distinct yet interconnected roles in maintaining health. While cholecalciferol is essential for bone health and immune function, cholesterol is crucial for cell membrane integrity and hormone synthesis. Understanding their mechanisms of action, appropriate usage, potential side effects, and drug interactions is vital for optimizing health outcomes and minimizing risks. As always, individuals should consult healthcare professionals for personalized advice and monitoring, especially when using supplements or medications.
Cholecalciferol Chloesterol Introduction:
Cholecalciferol, sold under various trade names such as D3-Max, Bio-D-Mulsion, and Calcirol, targets the vitamin D receptors (VDR) in the body. It is primarily used to treat and prevent vitamin D deficiency, which can lead to bone disorders such as rickets in children and osteomalacia in adults. Research institutions across the globe have been investigating the broader implications of vitamin D, including its role in immune function, cardiovascular health, and even cancer prevention. Cholecalciferol is available in various forms, including tablets, capsules, and liquid drops, and can be obtained both over-the-counter and through prescription.
Cholesterol, though often vilified due to its association with cardiovascular disease, is an essential molecule in the body. It serves as a building block for cell membranes, hormones (such as estrogen and testosterone), and bile acids, which aid in fat digestion. Cholesterol is synthesized in the liver and can also be obtained from dietary sources. It is important to distinguish between high-density lipoprotein (HDL) cholesterol, which is considered "good," and low-density lipoprotein (LDL) cholesterol, which is considered "bad" because high levels can lead to plaque buildup in the arteries.
Cholecalciferol Chloesterol Mechanism of Action:
Cholecalciferol is converted in the liver to 25-hydroxyvitamin D (calcidiol), the major circulating form of vitamin D. Calcidiol is then converted in the kidneys to its active form, 1,25-dihydroxyvitamin D (calcitriol). Calcitriol binds to vitamin D receptors (VDR) in various tissues, including the intestines, bones, and kidneys, to regulate calcium and phosphate metabolism. This action is crucial for maintaining healthy bone structure and mineralization.
Cholesterol metabolism is a complex process involving multiple pathways. Cholesterol is synthesized in the liver through a multi-step process that begins with acetyl-CoA and involves the enzyme HMG-CoA reductase, a key regulatory step in cholesterol synthesis. Cholesterol can be transported in the bloodstream by lipoproteins, including HDL and LDL. HDL is responsible for transporting cholesterol from peripheral tissues back to the liver for excretion, a process known as reverse cholesterol transport. In contrast, LDL carries cholesterol to peripheral tissues, where it can be used for cell membrane synthesis and hormone production.
How to Use Cholecalciferol Chloesterol:
Cholecalciferol is typically administered orally in the form of tablets, capsules, or liquid drops. The dosage varies depending on the individual's age, health status, and the severity of vitamin D deficiency. For example, the recommended dietary allowance (RDA) for adults ranges from 600 to 800 IU (international units) per day, while higher doses may be prescribed for individuals with severe deficiency or certain medical conditions. It is generally advised to take cholecalciferol with a meal containing fat to enhance absorption, as vitamin D is fat-soluble.
The onset of action for cholecalciferol can vary. While it may take several days to weeks for serum 25-hydroxyvitamin D levels to rise significantly, the clinical effects on bone health and calcium metabolism may take several months to become apparent. Regular monitoring of vitamin D levels and calcium status is recommended during supplementation to ensure efficacy and safety.
Cholesterol levels can be managed through lifestyle modifications, dietary changes, and medication if necessary. Statins are the most commonly prescribed drugs for lowering LDL cholesterol levels. These medications inhibit HMG-CoA reductase, the enzyme involved in cholesterol synthesis in the liver. Other lipid-lowering agents include bile acid sequestrants, niacin, and fibrates, which target different aspects of cholesterol metabolism.
What is Cholecalciferol Chloesterol Side Effects:
Cholecalciferol is generally well-tolerated when taken at recommended dosages. However, excessive intake can lead to hypervitaminosis D, a condition characterized by elevated levels of vitamin D in the blood. Symptoms of hypervitaminosis D include hypercalcemia (high levels of calcium in the blood), which can cause nausea, vomiting, weakness, frequent urination, and kidney stones. Severe hypercalcemia can lead to more serious complications such as arrhythmias and kidney failure.
Contraindications for cholecalciferol use include hypercalcemia, vitamin D toxicity, and certain conditions such as sarcoidosis and primary hyperparathyroidism, where patients may already have elevated levels of calcium or vitamin D. Individuals with kidney disease should also use cholecalciferol cautiously, as their ability to convert vitamin D to its active form may be impaired.
Cholesterol-lowering medications, particularly statins, can also have side effects. Common side effects of statins include muscle pain, fatigue, and digestive problems. Rare but serious side effects include liver damage, myopathy (muscle disease), and increased risk of type 2 diabetes. Patients on statins should have their liver function monitored regularly.
What Other Drugs Will Affect Cholecalciferol Chloesterol:
Several drugs can interact with cholecalciferol, affecting its absorption, metabolism, or efficacy. For example, corticosteroids can reduce calcium absorption and impair vitamin D metabolism, potentially necessitating higher doses of cholecalciferol. Orlistat, a weight-loss medication, can reduce the absorption of fat-soluble vitamins, including vitamin D. Anticonvulsants such as phenytoin and phenobarbital can increase the metabolism of vitamin D, leading to lower serum levels.
Cholesterol-lowering medications can also interact with other drugs. Statins, for example, are metabolized by the liver enzyme CYP3A4. Drugs that inhibit this enzyme, such as certain antibiotics (e.g., clarithromycin), antifungal agents (e.g., ketoconazole), and grapefruit juice, can increase statin levels in the blood, raising the risk of side effects. Conversely, drugs that induce CYP3A4, such as rifampin, can reduce statin levels and efficacy. Additionally, combining statins with other lipid-lowering agents like fibrates can increase the risk of muscle-related side effects.
In conclusion, cholecalciferol (vitamin D3) and cholesterol play distinct yet interconnected roles in maintaining health. While cholecalciferol is essential for bone health and immune function, cholesterol is crucial for cell membrane integrity and hormone synthesis. Understanding their mechanisms of action, appropriate usage, potential side effects, and drug interactions is vital for optimizing health outcomes and minimizing risks. As always, individuals should consult healthcare professionals for personalized advice and monitoring, especially when using supplements or medications.
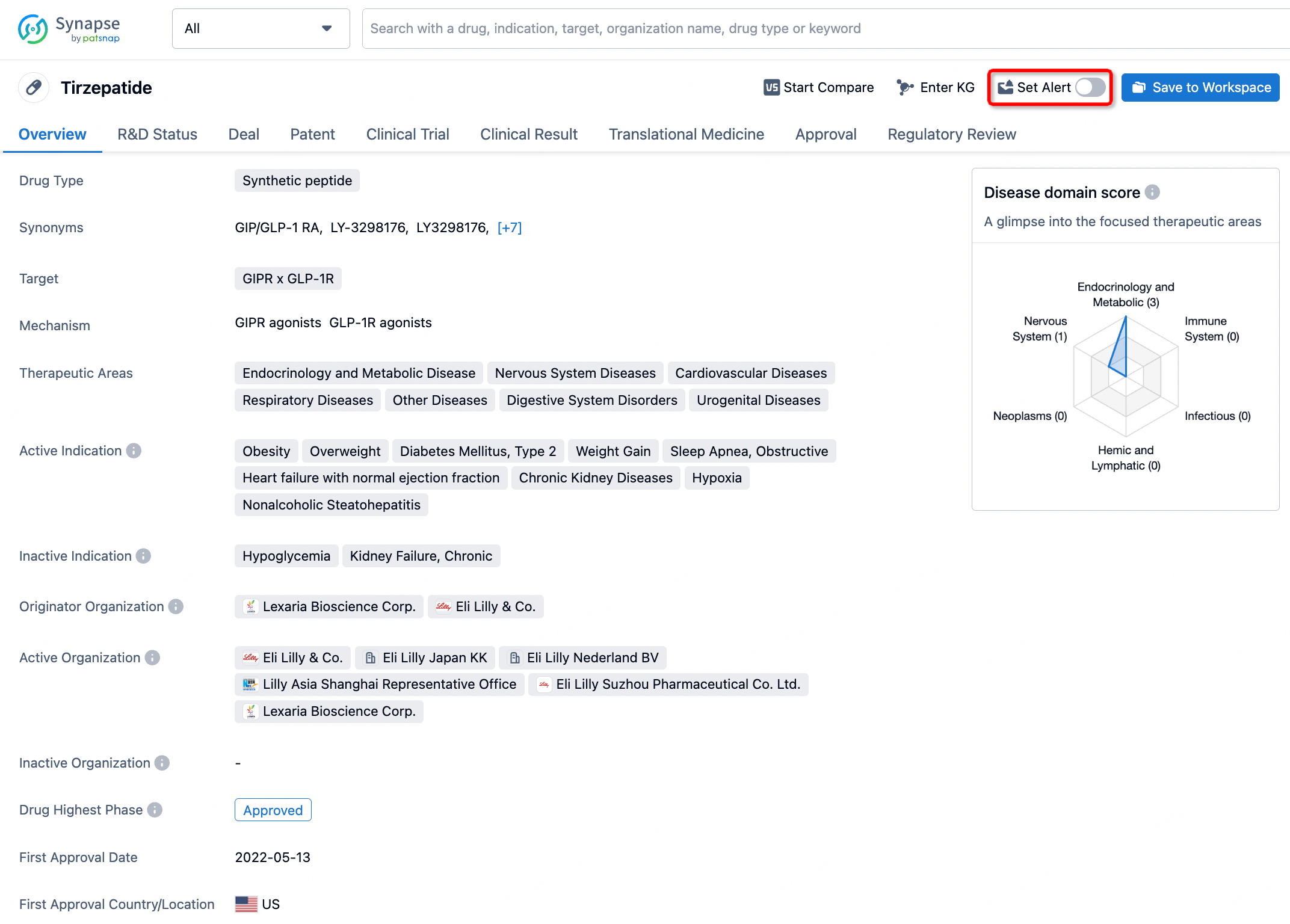
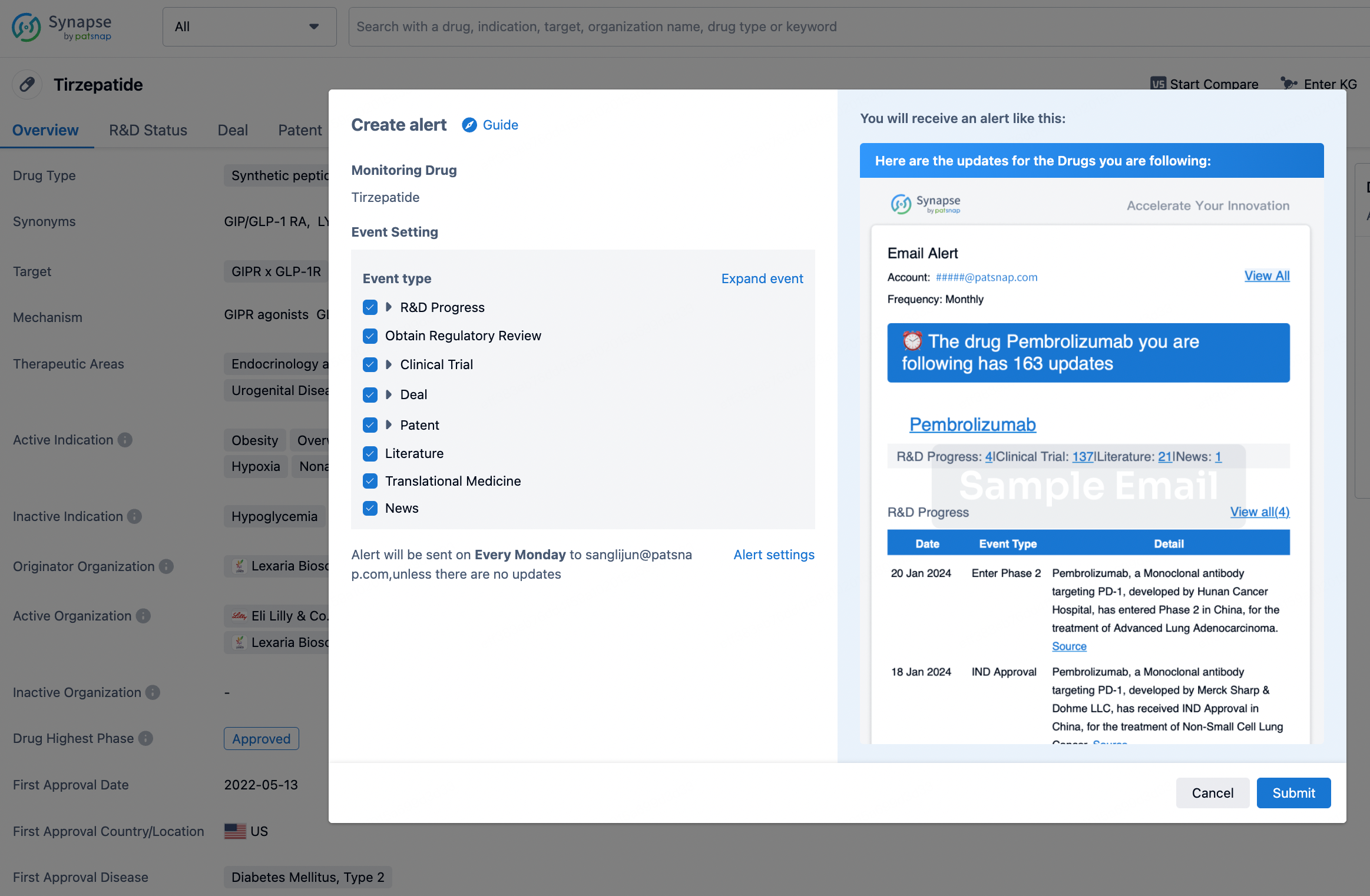
How to obtain the latest development progress of all drugs?
In the Synapse database, you can stay updated on the latest research and development advances of all drugs. This service is accessible anytime and anywhere, with updates available daily or weekly. Use the "Set Alert" function to stay informed. Click on the image below to embark on a brand new journey of drug discovery!
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.